Every child with spinal muscular atrophy (SMA) is affected differently. Age of onset, symptoms, characteristics of SMA and disease severity differ greatly from one child to the next.1
The characters shown are real patients and the required consent to use their stories has been obtained from the patients and families. Photographs are for illustrative purposes only.
Share page
SPINAL MUSCULAR ATROPHY IN INFANTS & CHILDREN
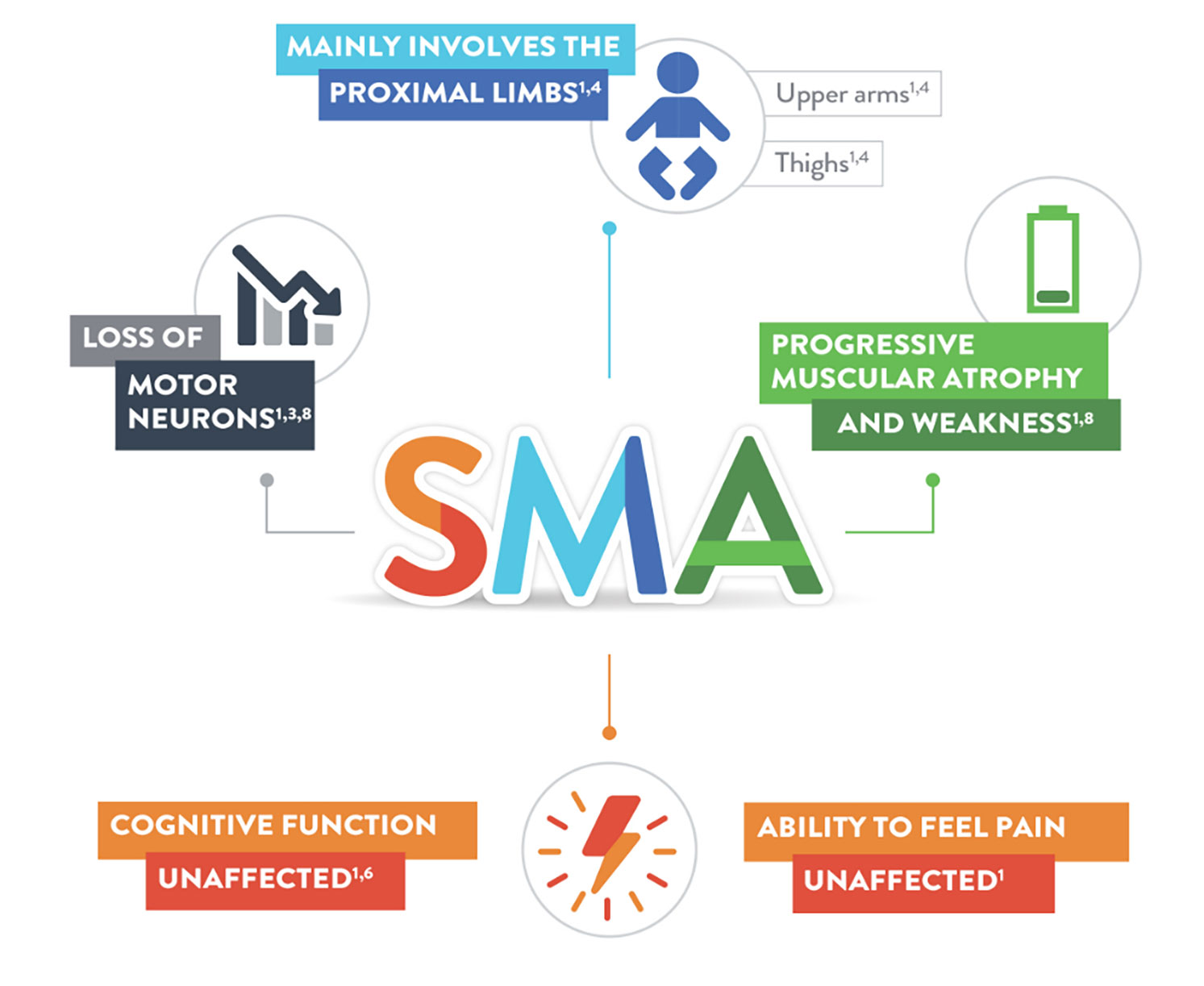
SMA is a rare, genetic neuromuscular disease1,2 and a leading genetic cause of infant and toddler mortality.3
Children may experience progressive muscle weakness in the muscles closest to the centre of the body, such as the shoulders, thighs, and pelvis. These muscles enable activities such as crawling, walking, sitting up, and controlling head movement. Their ability to breathe and swallow may also be affected.4
SMA does not affect the neurons responsible for cognition, which is the mental process through which we gain knowledge and understanding through thought, experience, and the senses.5.6
According to one study, children and adolescents with SMA have normal intelligence, with IQs in the standard range.7
Share now
SMA AFFECTS EVERY CHILD DIFFERENTLY
Symptoms may include progressive muscle weakness, floppiness, and muscle wasting (atrophy). Muscle weakness is usually the same on both sides of the body.9
Each child may experience symptoms differently, and the disease is divided into types based on age of onset and functional ability. There is also a range of severity within each type, and as many as 25% of individuals may not have a precise type.10
Share now
Share now
MISSING CERTAIN MILESTONES MAY BE THE FIRST SIGN OF SMA
Spinal muscular atrophy is often first suspected by a parent who may notice that their child is not meeting certain milestones. Parents may observe that their child is not reaching typical physical milestones for their age, such as the ability to hold their head up, to roll over, or to sit up independently.
Swallowing or feeding may also become difficult, and children may lose the ability to swallow safely without choking or inhaling food into the lungs (aspiration).5,11
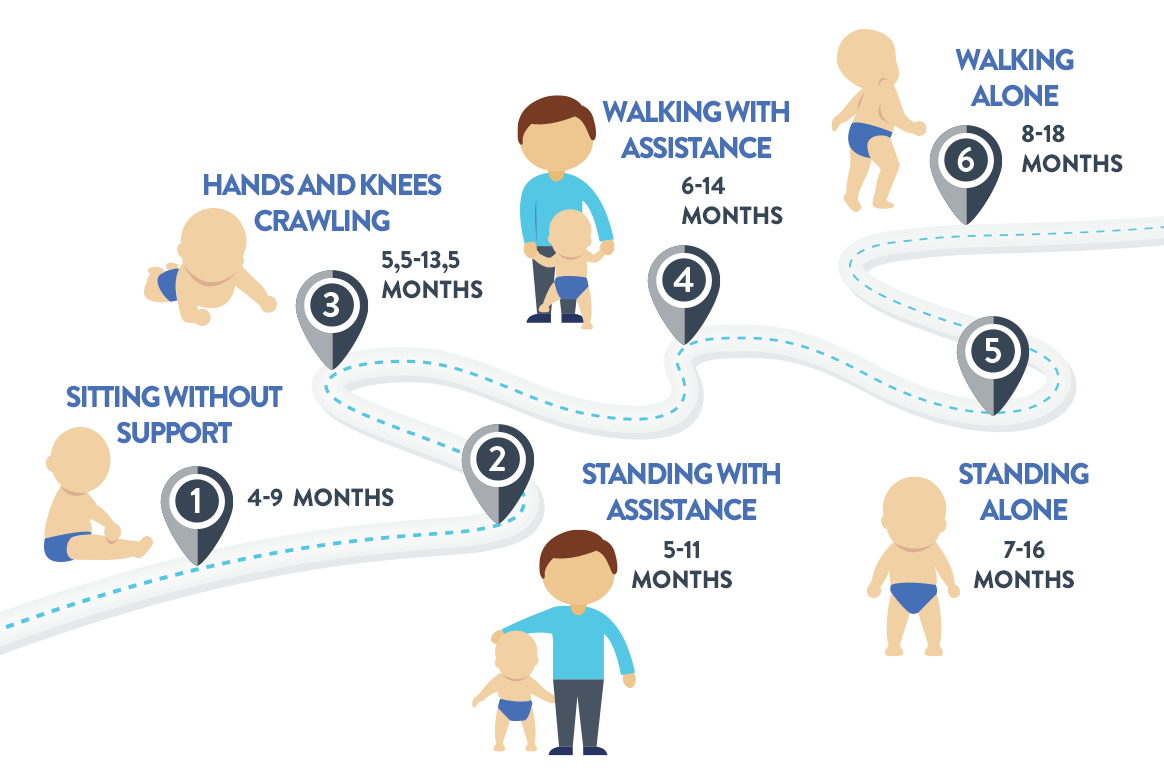
While all babies develop at their own pace, the World Health Organization (WHO) offers general motor milestone guidelines as part of the Multicentre Growth Reference Study (MGRS).12
Share now
Share now
Adapted from WHO Multicentre Growth Reference Study Group, 200613
MOTOR MILESTONE GUIDELINES12
GROSS MOTOR MILESTONE
PERFORMANCE CRITERIA
1.Sitting without support
Child sits up straight with head erect for ≥ 10 seconds.
Does not use arms or hands to balance body or support position.
2.Crawling on hands and knees
Child moves forward or backward on hands and knees.
The stomach does not touch the supporting surface.
Continuous and consecutive movements, ≥ 3 in a row.
3.Standing with assistance
Child stands in upright position on both feet, holding on to a stable object, such as furniture.
Child stands holding on for ≥ 10 seconds.
4.Walking with assistance
Child is in upright position with back straight.
Makes sideways or forward steps holding on to stable object with one or both hands.
One leg moves forward while the other supports body weight.
Child takes ≥ 5 steps.
5.Standing alone
Child stands in upright position on both feet (but not on the toes) with the back straight.
The legs support 100% of the weight, without holding on, for ≥ 10 seconds.
6.Walking alone
Child takes ≥ 5 steps independently, with the back straight.
One leg moves while the other supports most of the weight.
There is no contact with a person or object.
Share now
CHARACTERISTICS OF SMA IN INFANTS AND CHILDREN
Find out more about the characteristics and different types of SMA at various ages of onset:
Can hold head up and begins to push up when lying on stomach; makes smoother movements with arms and legs.
4 months:
Holds head steady, unsupported; pushes down on legs when feet are on a hard surface; may be able to roll over from stomach to back; can hold a toy and swing it at dangling toys; brings hands to mouth; when lying on stomach, pushes up to elbows.
6 months:
Rolls over in both directions (front to back and back to front); begins to sit without support; when standing, supports weight on legs and might bounce; rocks back and forth, sometimes crawling backwards before going forward.
Highest motor milestone achieved
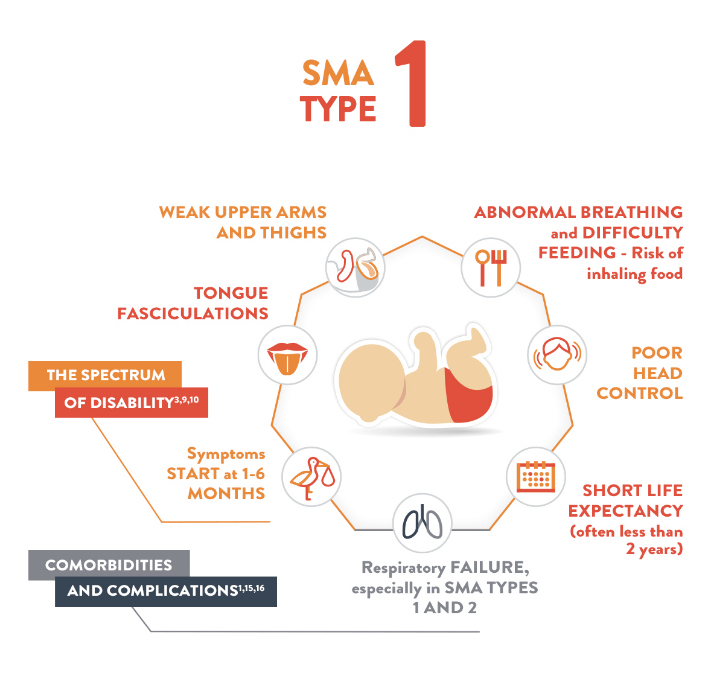
Unable to sit (“non-sitters”)
Life expectancy
≤ 2 years14
SMA Type
Type 1 (also known as Werdnig-Hoffmann disease)
Characteristics:14,17,18
Poor head control
Weak cough
Weak cry
Progressive weakness of muscles used to chew and swallow
Poor muscle tone
“Frog-leg” posture when lying
Severe muscle weakness on both sides of body
Progressive weakness of muscles that help in breathing (intercostal muscles), resulting in the characteristic “bell-shaped” chest
Share now
DEVELOPMENTAL MILESTONES:11
9 months:
Stands, holding on; can get into a sitting position; sits without support; pulls to stand; crawls.
1 year:
Gets into sitting position without help; pulls up to stand, walks holding onto furniture (cruising); may take a few steps without holding on; may stand alone.
Highest motor milestone achieved
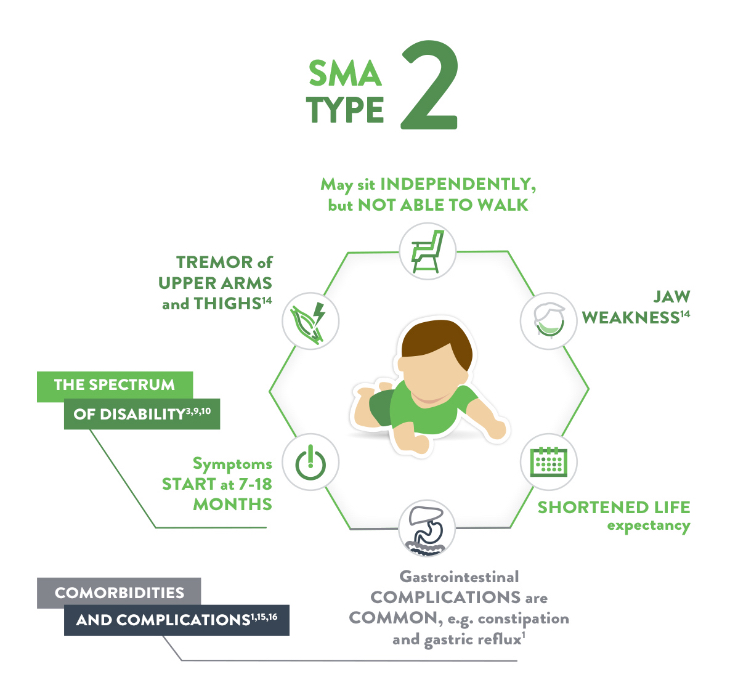
Able to sit independently (“sitters”)
Life expectancy
> 2 years14
70% still living at age 25
SMA Type
Type 2 (also known as Dubowitz disease)
Characteristics:17, 18
Muscle weakness
Swallowing, coughing, and breathing problems may occur but are typically less common
Muscle aching and joint stiffness symptoms
Children may develop spinal problems such as scoliosis (curvature of the pine), which may require bracing or surgery
Share now
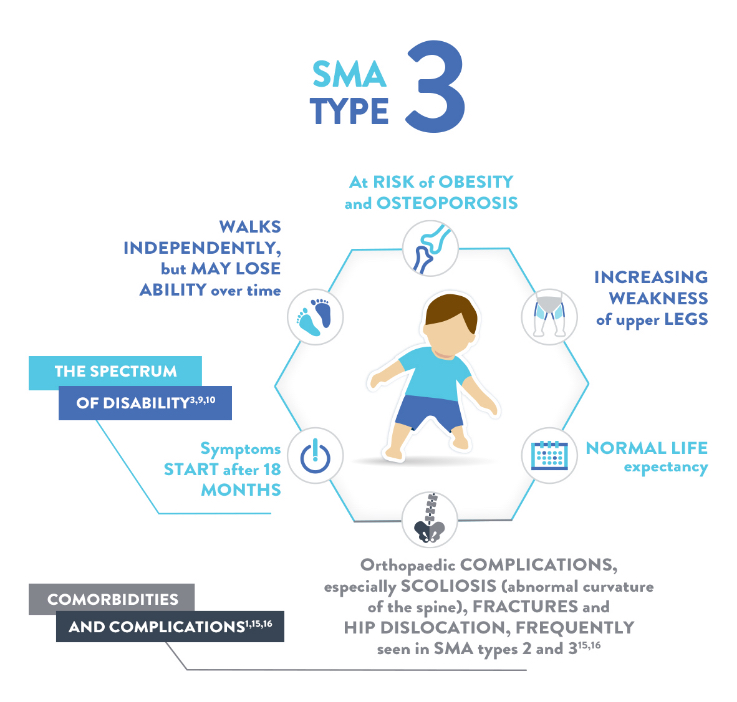
Highest motor milestone achieved
Able to walk independently (“walkers” - although they may progressively lose this ability)
Life expectancy
Normal14
SMA Type
Type 3 (also known as Kugelberg-Welander disease)
Characteristics:17, 18
Scoliosis
Chewing and swallowing difficulty
Muscles in the legs are generally more severely affected than the arms
Physical symptoms are similar to juvenile-onset spinal muscular atrophy, with the gradual onset of weakness, tremors, and muscle twitching first noted in late teens or early adulthood
Share now
Share now
Share now
LISTEN TO LAMONT’S FAMILY PERSPECTIVE
“Time to diagnosis is very important because it helps the families to get the types of supports they need.”
– Lilah’s mum
Watch video nowvideoWrapper1
Parents’ reports of their children’s gross motor development tend to be reliable. Sharing observations of potential motor delays with a doctor can help determine an appropriate care strategy.19,20
The characters shown are real patients and the required consent to use their stories has been obtained from the patients and families. Photographs are for illustrative purposes only.
References
1. Wang CH, et al. Consensus statement for standard of care in spinal muscular atrophy. J Child Neurol. 2007;22(8):1027-1049.
3. Lunn MR, Wang CH. Spinal muscular atrophy. Lancet. 2008;371(9630):2120-2133.
4. Finkel R, et al. 209th ENMC International Workshop: Outcome Measures and Clinical Trial Readiness in Spinal Muscular Atrophy 7-9. November 2014, Heemskerk, The Netherlands. Neuromuscul Disord. 2015;25(7):593-602.
5. Qian Y., McGraw S., Henne J., Jarecki J., Hobby K., Yeh W.S. Understanding the experiences and needs of individuals with Spinal Muscular Atrophy and their parents: A qualitative study. BMC Neurol. 2015;15:1–12. doi: 10.1186/s12883-015-0473-3.
7. Von Gontard et al. Intelligence and cognitive function in children and adolescents with spinal muscular atrophy. Neuromuscul Disord. 2002. Feb;12(2):130-6.
11. Centers for Disease Control and Prevention. Developmental milestones. Available at: http://www.cdc.gov/ncbddd/actearly/milestones/. Updated January 21, 2016. Accessed April 27, 2016.
12. Wijnhoven TMA, de Onis M, Onyango AE, et al; for the WHO Multicentre Growth Reference Study Group. Assessment of gross motor development in the WHO Multricentre Growth Reference Study. Food Nutr Bull. 2004;25(1 suppl 1):S37-S45.
14. Markowitz JA, Singh P, Darras BT. Spinal muscular atrophy: a clinical and research update. Pediatr Neurol. 2012;46(1):1-12.
15. Haaker G, Fujak A. Proximal spinal muscular atrophy: current orthopedic perspective. Appl Clin Genet 2013;6:113-120.
16. Darras BT. Spinal muscular atrophies. Paediatr Clin North Am 2015;62(3):743-766. DOI: 10.1016/j.pcl.2015.03.010.
17. Mercuri E, et al. Diagnosis and management of spinal muscular atrophy: Part 1: Recommendations for diagnosis, rehabilitation, orthopedic and nutritional care. Neuromuscl Disord. 2018;28(2):103-115.
18. Prior TW, Russman BS. Spinal muscular atrophy. NCBI Bookshelf Website. Available at: http://www.ncbi.nlm.nih.gov/books/NBK1352/. Updated November 14, 2013. Accessed April 15, 2016.
19. Noritz GH, Murphy NA; and Neuromuscular Screening Expert Panel. Motor delays: early identification and evaluation. Pediatrics. 2013;131(6):e2016-e2027.
20. Lawton S, Hickerton C, Archibald AD, McClaren BJ, Metcalfe SA. A mixed methods exploration of families’ experiences of the diagnosis of childhood spinal muscular atrophy. Eur J Hum Genet. 2015;23(5):575-580.